

Sustainable Healthcare Coalition
DIA
n 2021, ClinicalTrials.gov listed approximately 350,000 registered trials. That same year, a call to action in The Lancet highlighted the need for collaboration to decarbonize clinical trials and led the Sustainable Healthcare Coalition (SHC) to develop a tool to measure the carbon footprint of clinical trials and highlight hotspots, gauge progress, and benchmark work to reduce associated emissions. Although the tool has been developed, a number of important questions remain about its widespread use and meaningful impact.
The launch of this calculator coincided with the publication of an open letter by the CEOs of the member companies of the Sustainable Markets Initiative Health Systems Task Force which encouraged contract research organizations to measure emissions for all phase 2 and 3 clinical trials beginning in 2025, in line with the Task Force’s own commitment to do the same.
Considering these efforts alongside the European Commission’s expectation of a 90% reduction of the EU’s greenhouse gas emissions by 2040, we must ask:
- Where does the clinical research industry in Europe currently stand in relation to this target, and what will it take for clinical trials in Europe to reach it?
- How can stakeholders in this diverse ecosystem share their accumulated knowledge and learn from each other for the purpose of reducing greenhouse gas emissions?
- Can we learn from the accelerated action surrounding clinical trial diversity and inclusion initiatives and apply these lessons to sustainability?
This article summarizes discussions from the November 2024 Sustainable Clinical Trials Think Tank jointly organized, hosted, and presented in Amsterdam by DIA and the Sustainable Healthcare Coalition (SHC).
Carbon Footprint Data
Measuring impact is the first step towards meaningful change, and early data on the carbon footprint of clinical trials are becoming available. It is important to use data to challenge or support our preconceptions of decarbonizing activities. For example, do the decarbonization benefits of adopting digital solutions outweigh their inherent carbon emissions? Standardizing and harmonizing the collection of these data is also critical to ensure a coherent effort. Eventually, these data could refine the modeling tool that predicts the emissions of clinical trials and may eventually demonstrate that sustainability isn’t necessarily an additional burden on the system but actually leads to cost reductions.
It is important to recognize that the “Global South” is not well represented in the available data, and data collected from the “Global North” are rarely translatable to the South due to differences in socioeconomic, political, and cultural contexts. It is essential, in line with the fundamental principle of health equity and to prevent further disparity and disconnect, to integrate the Global South and the rest of the world in sustainability initiatives and interventions.
Discussants suggested that the carbon footprint of an activity or product could be considered as a debt that needs to be reimbursed further downstream, for example by having a positive impact on societal values or an overall improvement to public health.
Despite a perceived expectation that society wants regulators and policy makers to start establishing rules and guidelines for sustainability, the group agreed that other approaches may be more efficient and less resource intensive. Carbon footprint data standards could be established through an international standards agency, for example, and a statement of intention from regulators which discloses their interest in carbon footprint data may have the intended effect without being as burdensome as a new regulation. (See Outcome-Based Cooperative Regulation or the Low Carbon Clinical Trials Working Group as examples.) It may be better for industry to proactively determine these standards instead of waiting for regulatory guidance or other direction.
The UK’s Greener NHS Net Zero Supplier Roadmap was identified as an excellent template from which to learn.
Tangible Measures to Reduce Clinical Trial Emissions and Eliminate Waste
Think tank discussants identified several tangible steps to maximize efficiencies and reduce clinical trial emissions:
- Decentralizing clinical trials and conducting virtual meetings and remote inspections/monitoring to reduce trial-related travel for site staff and patients
- When these cannot be conducted virtually/remotely, locating the meetings in places reachable by public transportation that uses renewable energy sources
- Minimizing travel by working with local sites, CROs/CRAs, and laboratories
- Avoiding multiple trials competing for similar patient populations at the same site
- Equipping trial sites with renewable energy and developing “green certifications” for sites
- Using real-world evidence and synthetic placebo arms to reduce the number and size of trials
- Employing digital enablers, ranging from digital twins to eLabeling, and using AI to consolidate and streamline logistics (shipping, etc.)
- Rethinking sample storage temperatures and durations
- Emphasizing the value of or incentivizing material recycling and repurposing (reusable shipping containers, etc.)
- Assessing the environmental impact of current clinical trial regulations
- Identifying sustainability-driving innovations that are at odds with existing regulatory policies and dialoguing with regulators to resolve these issues
- Negotiating with regulators for their acceptance of “softer” endpoints that generate fewer emissions
- Identifying and equipping designated “sustainability ambassadors” across stakeholder groups
- Storing and exchanging electronic data in the European health data space on servers in Europe instead of other locations.
Different Stakeholders and Roles
Education is necessary to accelerate sustainability, and knowledge sharing across all stakeholders is crucial. Sharing knowledge from patient associations, for example, may enable collecting and analyzing patient travel data to determine the environmental impact of their travel.
A patient-centric approach to decentralized clinical trials (DCTs) will balance emissions with patient benefits. We are nearing the point where we can measure the carbon emission difference that is due to decentralization. Are the benefits of decentralization to the patient “worth” the difference?
Other stakeholders in the clinical trial ecosystem, such as developers of generics and biosimilars, may have different perceptions of the relationship between sustainability and cost efficiency. Linking sustainability to other success factors such as improved patient access and supply chain resilience would be a good way to increase the impact of current measures and expand the number of engaged stakeholders and their support for sustainability initiatives. The Health Technology Assessment (HTA) community, for example, has expressed interest in including elements of sustainability in HTA assessments.
The Learning Journey
Building communities of practice was identified as one efficient way to accelerate sustainability in clinical trials. Such communities of practice could identify barriers to building environmental sustainability into clinical trials and communicate them to regulators and other stakeholders, eventually contributing to greater compliance with directives and requirements.
It is critical to recognize the role of low- and middle-income countries (LMICs, or the “Global South” mentioned above) in this journey: Clinical trial frameworks in these nations often use fewer resources, and generate less waste and emissions, out of economic necessity, and may hold valuable lessons for stakeholders in the “Global North.”
The size of a company can impact its ability to implement and sustain sustainability measures. On the one hand, smaller companies are often able to more quickly and collaboratively change direction compared to larger ones; on the other, a recent SME Climate Hub survey showed that small and medium-sized businesses do not have as many financial and other resources to invest in these efforts. Data that links cost saving to sustainability measures will promote the financial benefits of sustainability to companies of every size.
Improved access to information for/from patients could have important impacts on sustainability:
- Failed patient recruitment efforts and sites have been identified as a major source of clinical trial waste.
- Increasing the role of patients in planning/designing clinical trials, and increasing communication between physicians/general practitioners and patients, may reduce waste and address other challenges in patient recruitment.
- Easier access to trial information could allow patients to enroll more easily and stay in trials longer because they would be more aware of options regarding location, travel, and related logistics.
- Trial exit surveys can collect additional data from patients such as travel information and how they use digital tools while also providing trial teams with a vehicle to thank patients for their participation.
- Lessons can also be learned from specific therapeutic areas (e.g., infectious disease, respiratory, cardiovascular) because clinicians are already seeing the impact of climate change on these patients.
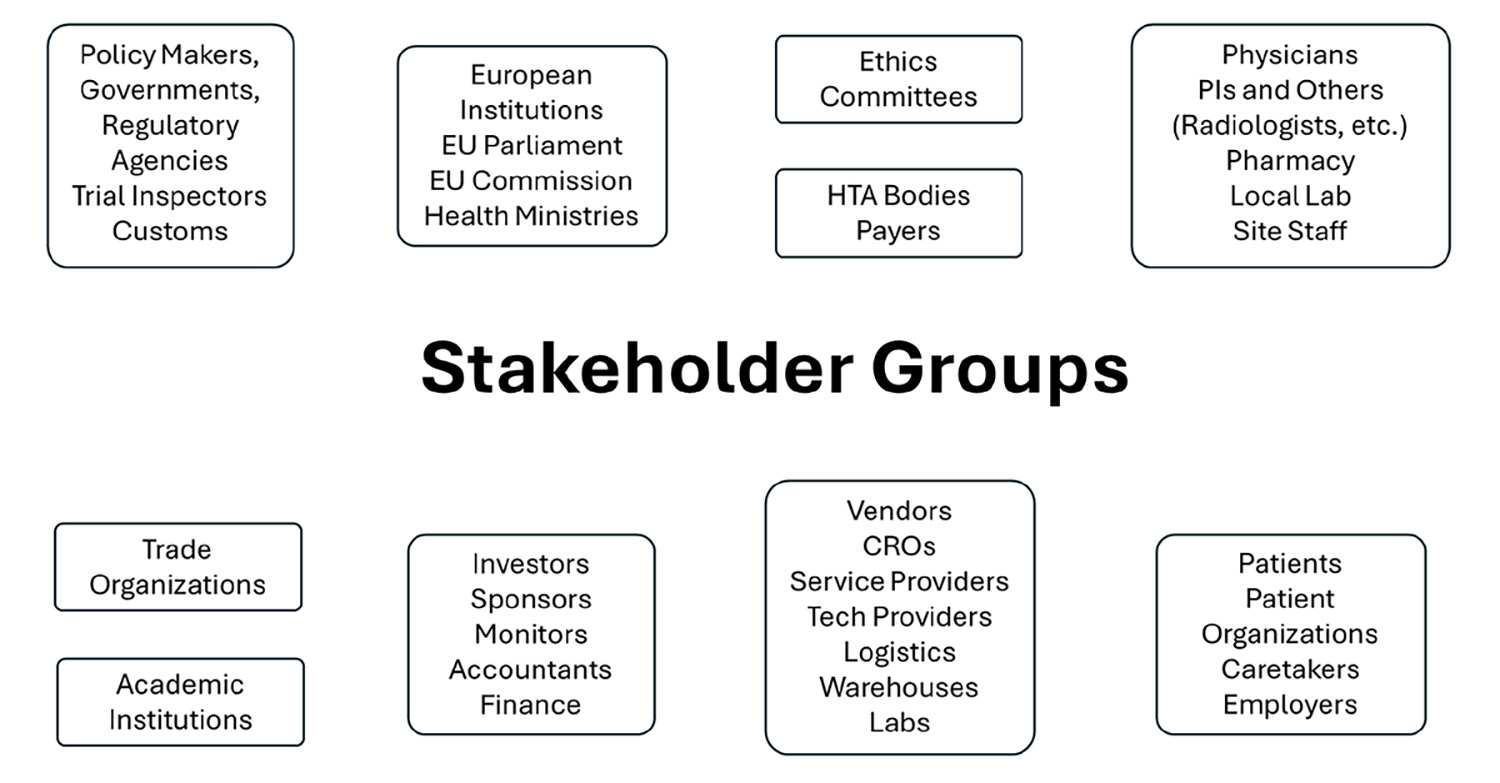
In this discussion, participants identified these stakeholder groups as having roles in reducing clinical trial carbon emissions:
- Create a clinical trial community of sustainability practice: Integrate organizations of all sizes and build working groups based upon functions/roles to allow the sharing of practice and ways to overcome common challenges.
- Create a communication channel between trial sponsors and regulators: Keeping regulators engaged in sustainability questions and solutions will help regulators understand where best practice currently is and where it is going, which will positively impact regulatory expectation and policy.
- Create a communication channel for systematic, comprehensive collaboration with physicians/general practitioners to help them find the right trials for their patients.
- Reduce barriers to patient access and increase awareness to make it easier for patients to find clinical trials.
- Partner with academic institutions to train the next generation on conducting trials in a more sustainable way.
Removing Barriers and Establishing Incentives
The first and most important barrier to change is mindset. Clear communication and understanding of the need for sustainability solutions for clinical trials will overcome this barrier. This leads to the second: the technical, technological barrier of knowing specifically where and how to reduce clinical trial emissions.
Collaborating with stakeholders responsible for one specific task on a large scale can help here. For example, the individual in charge of all shipments across all programs will understand the benefits that can come from optimizing this task better than the individual responsible for “optimizing clinical operations” as a whole.
Other major barriers include:
- The perception that sustainability measures and regulatory requirements are incompatible
- A lack of initiative and coordination (such as waiting for someone else to “take the first step”), and of an obligation to act, and lack of accountability, responsibility, and agency among stakeholders.
- A lack of awareness of possible solutions; of knowing what other stakeholders have tried or what works
- The perception that incorporating sustainability will negatively impact the time, cost, quality, or outcomes of a clinical trial
- A lack of economic models and bandwidth for investing resources in new sustainability solutions.
The group’s follow-on recommendations on how stakeholders can work together to remove these barriers included both short- and long-term actions:
- Expanding the frequency of sustainability collaborations and partnerships, as well as making them more global and more local
- Defining key sustainability indicators (KSIs) that standardize how to recognize success
- Using AI for data analysis to accelerate reducing emissions from clinical trials
- Sponsors, regulators, and payers collaboratively developing (and requiring) carbon emission reduction guidelines
- Developing a core communication plan, then tailoring communications for different stakeholders/geographies and disseminating them through networks, collaborators, and ambassadors
- Collaborating with the European Patients Academy on Therapeutic Innovation (EUPATI) to develop an environmental sustainability training program for patients
- Collaborating with academic institutions to train the new generation on sustainable clinical trials.
Participants also shared that there are few current incentives to encourage stakeholders to invest in sustainability initiatives, and suggested as possibilities:
- Integrating sustainability in clinical trial key performance indicators (KPIs) and in organizational environmental, societal, and governmental (ESG) and individual contributor objectives
- Establishing a “green label” to reward organizations (sponsors, vendors, etc.) with demonstrated investment in reducing their clinical trial emissions
- Celebrating “Green Champions” at various levels (organization, individual contributor, etc.)
- Incorporating sustainability into terms of procurement or other commercial negotiations
- Incentives for reinvesting CO2 savings.
Sustaining Sustainability
The Sustainable Healthcare Coalition is committed to establishing a community of practice that builds upon this think tank and is open to LMICs. We encourage all stakeholders to utilize the SHC’s clinical trials knowledge hub and to become a member of our community of practice. DIA is committed to introducing these think tank outcomes to the World Health Organization (WHO) and its partners for their assistance in developing sustainability considerations that can eventually be incorporated into good clinical practice.
DIA also invites you to learn more about its sustainability efforts at DIA Europe 2025.
True sustainability will eventually become a fourth item that expands the classic triad of project management: scope, cost, time—and sustainability.
We also thank workshop participants representing these other organizations or agencies: the Norwegian Medical Products Agency (DMP), Finnish Medicines Agency (FIMEA), Heads of Medicines Agencies Clinical Trials Coordination Group (HMA CTCG), Health Technology Assessment international (HTAi), the Medicines and Healthcare products Regulatory Agency (MHRA, UK), the South African Medical Research Council (MRC), and the University Hospital, Zürich.