

Institut de Recerca Sant Joan de Déu
ecentralized clinical trial elements include digital technologies such as telemedicine, remote monitoring, and real-time data collection to reduce reliance on in-person visits. While these innovations may improve accessibility and participant retention, they also introduce operational and coordination complexities for the teams managing different platforms and devices, as well as the need for training patients on these innovations with support from site staff.
What does it mean to decentralize a clinical trial?
A decentralized clinical trial (DCT) is a trial that implements strategies and technologies that reduce the dependence on in-person visits to research sites. Key elements of decentralization include:
- Telemedicine and virtual visits
- Remote patient monitoring
- Digital data collection
- Home nursing
- Home delivery of medication.
Pediatric Population Considerations
When conducting decentralized pediatric clinical trials, it is crucial to use age-appropriate technology (user-friendly interfaces and platforms), ensure informed consent of the minors and active participation of caregivers and patients, safeguard data privacy, and adhere to ethical standards. These measures enhance accessibility and efficiency while prioritizing the safety and well-being of children.
One-Stop-Shop Clinical Trials Unit
This article is based on analysis of 304 pediatric clinical trials conducted in the Clinical Trials Unit at SJD Barcelona Children’s Hospital from May 2022 to December 2024. These trials covered 17 therapeutic areas (oncology, neurology, neuromuscular diseases, dermatology, rheumatology, infectious diseases, immunology, nephrology, gastroenterology, hematology, endocrinology, pulmonology, Intensive Care Unit, psychiatry, traumatology, cardiology, and ophthalmology). At the time of this analysis, 769 patients were in treatment/follow-up.
This study evaluated each clinical trial to determine the number of electronic platforms that the trial coordinators had to manage and the number of devices (wearables) each trial included.
Eighty-five percent of the studies used electronic management platforms, for a total of 1611 electronic platforms. The studies also managed a total of 252 devices.
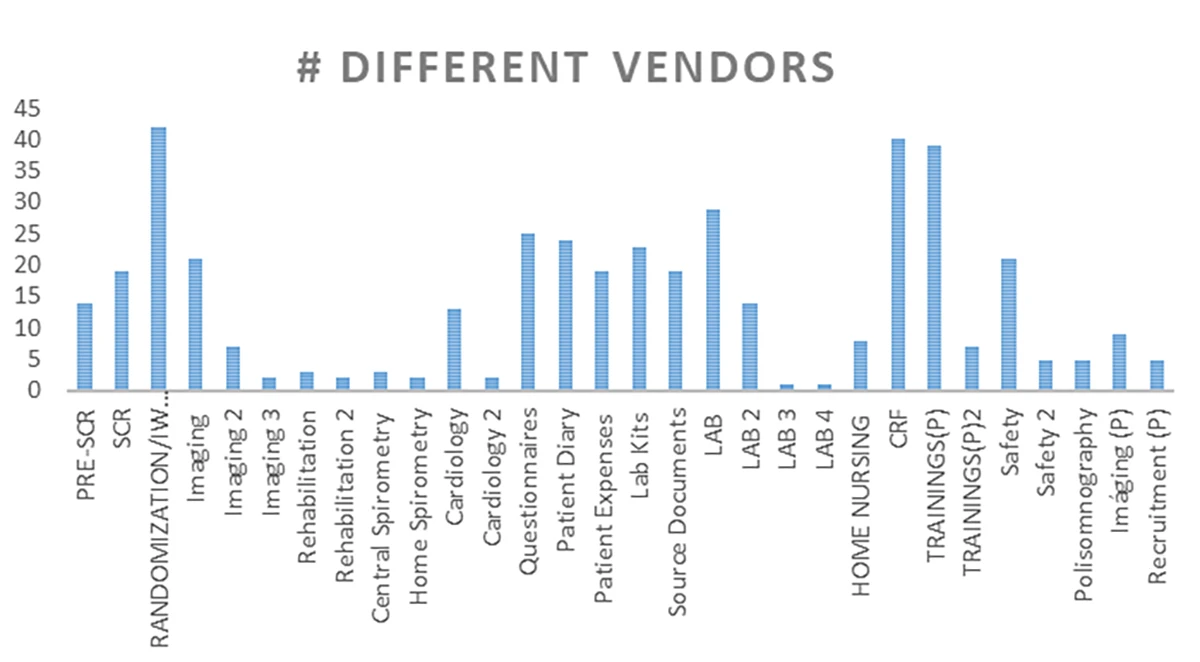
Closer data analysis shows that 30 different digital activities were carried out in the context of these trials (see Table 1):
Do We Spend More Time on Devices than on Patients?
An interesting dilemma has arisen. The amount of time that researchers spend on devices in the name of patients is increasing and has become one of the main points of debate in the transition to decentralized clinical trials: The implementation of advanced technology has allowed for more precise and accessible patient monitoring but has also raised concerns that human interaction in clinical research may be reduced.
This study assessed the total number of platforms, the number of different platforms, and the number of devices each coordinator managed in order to assess the impact of these technologies on their daily workload.
Number of Platforms Used by Clinical Trial Coordinators
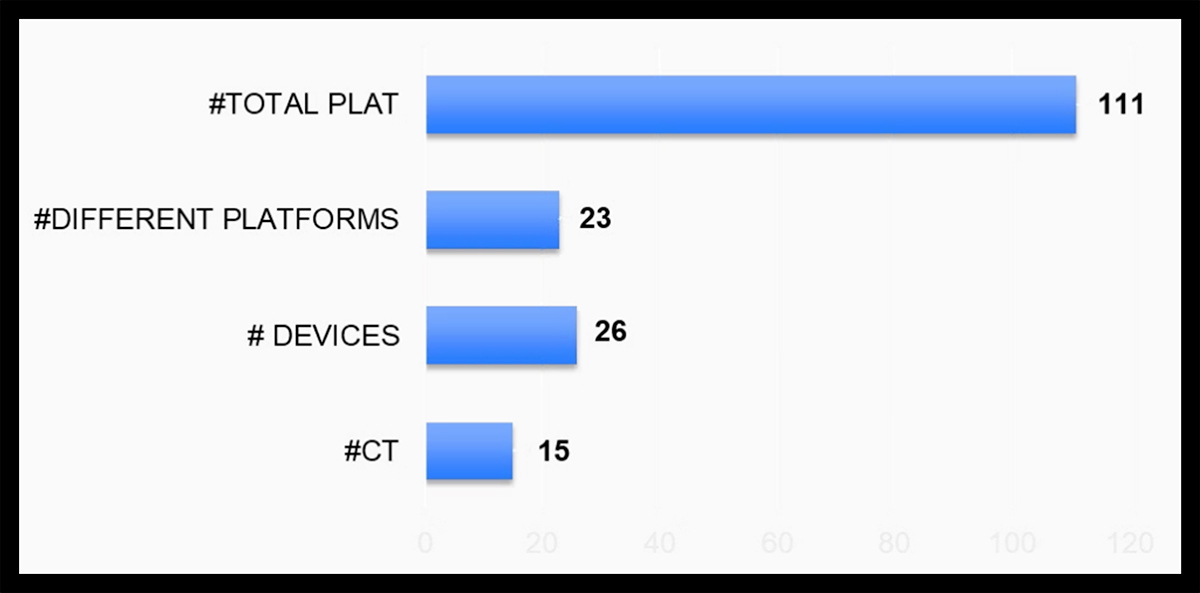
A research coordinator managing 15 clinical trials worked across 111 platforms (23 of which were unique and therefore lacked interoperability) alongside 26 devices (see Figure 1). Based upon these numbers, it seems reasonable to suspect that this workload shifted their focus from patient care to platform and device management.
Decentralized clinical trials aim to enhance efficiency and reduce physical visits but risk compromising interpersonal care without patient-centered designs. This is particularly challenging in pediatric trials, where in-person evaluations are vital. Wearable devices and platform integration further demand technical support to address complexities.
It should also be noted that the caregiver experience surveys that are completed at our own site showed that most parents of pediatric trial participants preferred in-person visits, valuing direct interaction and reassurance from healthcare providers over telemedicine.
Clear Benefits in Accessibility and Efficiency
Decentralization of clinical trials has genuinely transformed how research is conducted. Its benefits in terms of accessibility, patient inclusion, and data monitoring optimization are evident. Critical evaluation metrics include recruitment efficiency, population diversity, participant dropout rates, and adherence to protocols by principal investigators.
However, its implementation has generated a series of operational challenges that can lead to technology overload for research sites. While decentralization should facilitate patient participation, it also implies redefining the role of the research site, which must integrate new technologies, train staff on their use, and assume a greater coordination burden.
Decentralization of clinical trials also aims to optimize the integration of technological systems and human interaction to enable efficient clinical research and prevent research resource overuse. Innovative, advanced digital technologies such as real-time data acquisition, telemedicine, and remote monitoring systems enhance participant accessibility and retention while minimizing carbon emissions associated with physical site visits.
The production and operation of portable devices and electronic platforms require substantial energy and resource inputs, which may increase environmental impact if not properly mitigated. Research institutions must implement eco-conscious strategies, including device recycling and reliance on renewable energy sources, to mitigate these potential adverse effects. These conservation efforts also align with the United Nations’ Sustainable Development Goals (SDGs); specifically, Goal 13 to combat climate change and its impact.
Although decentralization offers substantial benefits in sustainability and accessibility, its efficacy varies significantly across different clinical trial scenarios. In this analysis, certain scenarios demonstrated clear advantages and benefits while others revealed challenges and limitations, underscoring the impracticality of universal implementation. Additionally, the proliferation of additional management platforms increases operational complexity and places new burdens on research management personnel.
Standardization and rationalization of platform usage are essential to streamline operations and maximize environmental and logistical benefits while maintaining scientific rigor. One relevant, if currently infeasible, recommendation is the development of a unique, single platform which centralizes and executes all clinical trial management needs.